

She stopped coming to the Wednesday Bible study about six months ago. Before that she had been faithful, quiet, always in the same seat near the door. People noticed the empty chair. Nobody called. There had been an incident a few weeks earlier. During the prayer time she had said something that made the room uncomfortable, something about voices, about messages she was receiving, about a reality that did not line up with the one everyone else was sitting in. The room had gone quiet. Someone prayed over her. Someone else suggested she speak to the pastor. She did not come back. What nobody understood was that she did not need a prayer ministry session and a pastoral conversation. She needed a hospital.
This is the fourth in a series on "What the Church Needs to Know about Mental Health".
This Is Not Split Personality
The most stubborn misconception about schizophrenia is buried in the name itself. The Greek roots suggest a splitting of the mind, and popular culture has turned that into the idea of a person with two or more personalities trading places. That is not schizophrenia. That is a different condition entirely. Schizophrenia is not about multiple selves. It is about a single self whose relationship with reality has been seriously disrupted.
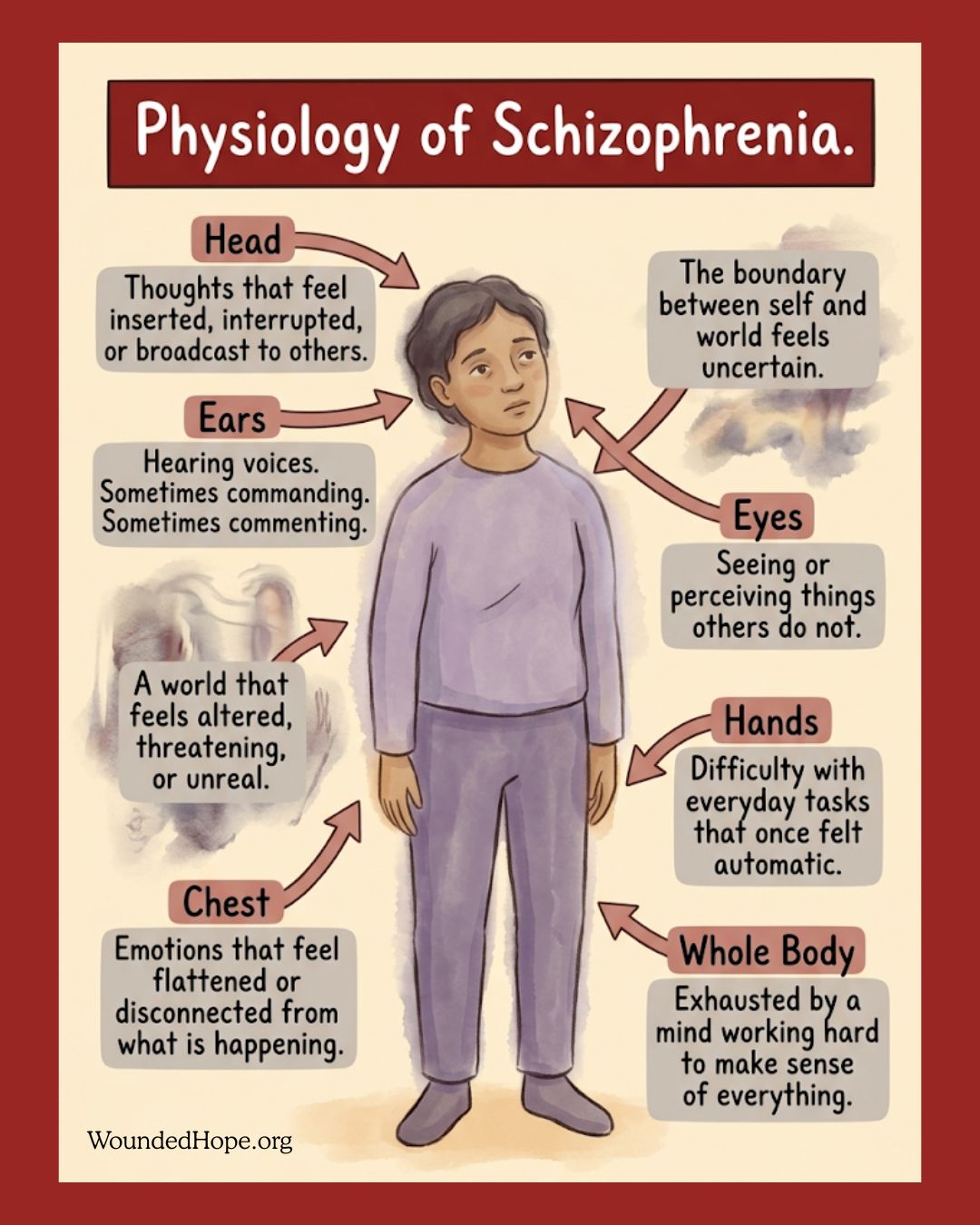
Schizophrenia is a serious, chronic mental illness affecting how a person thinks, perceives, and relates to the world. It tends to involve two categories of symptoms.
The first are sometimes called positive symptoms, meaning experiences added to a person's reality. Hallucinations, most often hearing voices that others do not hear. Delusions, which are fixed beliefs not grounded in shared reality and not movable by argument. And disorganised thinking, where the ordinary connections between thoughts break down in ways that make speech hard to follow.
The second are negative symptoms, meaning capacities reduced or stripped away. Flattened emotional expression. Reduced motivation. Withdrawal from people. Difficulty with the ordinary tasks of daily living that the rest of us do without thinking.
The condition usually emerges in late adolescence or early adulthood. It is not caused by trauma, by bad parenting, or by spiritual failure. It is a neurological condition with a strong genetic component, and it requires long-term psychiatric treatment and careful medication management. See accompanying infographic.
It is present in your congregation. Not commonly, but it is there. And how the church responds when it surfaces will either draw that person deeper into community or push them further into isolation, often at the worst possible moment.
Of all the conditions in this series, schizophrenia carries the heaviest theological misreading.
Hearing voices. Receiving messages from unseen sources. Perceiving a reality others cannot access. In many charismatic and evangelical settings, these experiences get interpreted through a framework of spiritual warfare or prophetic gifting long before anyone considers a medical explanation. The instinct is understandable. The categories feel close. But the consequences of reaching for the spiritual frame first are severe.
It does two specific and serious kinds of harm.
The first is delayed treatment, and this is not a small matter. Schizophrenia is a condition where early intervention significantly affects long-term outcomes. A person who begins psychiatric treatment near the onset of their first episode generally has a meaningfully better prognosis than one whose treatment is delayed by months or years. When a church responds to the early signs with prayer ministry, deliverance sessions, or a long process of spiritual discernment, it is not merely offering inadequate help. It is delaying the medical care the person urgently needs, and in some cases that delay causes lasting harm. This is the heart of the matter, and it is why this article exists. When someone is in psychiatric crisis, the most spiritual thing the church can do is help them get to a doctor.
The second harm is the message it sends about the condition itself. When a church treats schizophrenia as demonic oppression or spiritual attack, it tells the person and their family that what is happening is a moral or spiritual failure needing spiritual correction. That is theologically imprecise and pastorally devastating. A family already carrying a schizophrenia diagnosis does not need the added weight of believing their loved one is spiritually compromised. They need accurate information, practical support, and a community willing to walk a long road that will not resolve quickly.
The church does not have to choose between taking the spiritual life seriously and taking medical reality seriously. Both can be held at once. What cannot be held is a framework that substitutes spiritual explanation for medical care while someone is in crisis.
We return to Mark 5, because the passage holds more than one truth for this series.
The man among the tombs is experiencing something the text does not name in clinical terms but describes in ways that resonate with psychosis. Voices. An altered perception of reality. Behaviour others cannot contain or control. A complete severing from ordinary community life. He lives among the dead, isolated, beyond the reach of the chains the townspeople had used to manage him.
What Jesus does matters spiritually, and it also matters structurally.
He does not theologise the man's condition into a lesson. He does not require him to confess sin or prove his faith before being helped. He addresses what is in front of him, restores the man to himself, and returns him to community. And the instruction that follows the healing is striking. It is not come and join my public ministry. It is go home to your own people and tell them how much the Lord has done for you (Mark 5:19). The restored life begins in the ordinary. Family. Community. Daily existence. Not the spectacular, but the recovered.
And there is the detail about the townspeople, which is hard to ignore. They come out, find the man sitting there, clothed and in his right mind, and they are afraid (Mark 5:15). They ask Jesus to leave. They had organised their common life around managing this man's chaos, and his restoration unsettled the arrangement. Sometimes the church's discomfort around serious mental illness is not really fear of the condition. It is fear of what genuine restoration and genuine inclusion would actually ask of the community. Including someone in their ongoing reality is harder, and slower, than praying over them once and moving on.
If you are living with schizophrenia. Your experience is real to you, and you deserve to be treated with dignity, not managed from a distance or read through frameworks that do not fit your reality. The church has not always known how to hold what you carry, and that failure belongs to the church, not to you. You are not spiritually compromised. You are not beyond reach. You deserve accurate medical care, consistent community, and the ordinary belonging that Jesus gave the man among the tombs when he sent him home to his own people.
If you are a family member or carer. What you are carrying is one of the heaviest loads a family can bear. Schizophrenia is chronic, unpredictable, and widely misunderstood by the people around you. You need practical support, not theological explanations. You need someone to sit with you in the waiting room, help you navigate a confusing mental health system, and check on you after the hard appointments, not only on the person who is unwell. Your own wellbeing matters too. Carer burnout is real and serious, and tending to yourself is not a betrayal of the person you love. It is what makes it possible to keep loving them for the long haul.
If you are a pastor or church leader. Three things are needed here more urgently than almost anywhere else in this series. The first is basic psychoeducation for your pastoral team. Every pastor and elder should be able to tell the difference between a spiritual experience and a psychiatric symptom, not to replace discernment with diagnosis, but to know when someone needs a doctor before they need a deliverance session. The second is a clear referral pathway to psychiatric services. Know what is available locally. Have the numbers ready before you need them. Be willing to accompany a family to a first appointment. The third is a long-term commitment to inclusion. Schizophrenia does not resolve. The person who returns from a psychiatric admission is not cured; they are managing. What they need from the church is not a return to normal but a community that has learned to include them in their ongoing reality, not only in their crisis.
***
She has not come back to the Wednesday Bible study. She is in a different place now, steadier than she was, managing what she can with the support of a psychiatric team and a family that has slowly learned what she needs.
What she never found was a church that knew what to do when she said something that did not fit the room. The quiet that fell, the prayer that missed the point, the phone calls that never came, none of it was malice. It was ignorance. And ignorance, in this case, cost her the community she needed most in the hardest season of her life. The church can learn what it does not yet know. It can build the knowledge, the referral pathways, and the culture of inclusion, so that the next person who says something that does not fit the room is met not with silence but with the steady, informed, unglamorous love that knows when to pray, when to call a doctor, and how to walk someone all the way home.
Part 1 – Depression
Part 2 – Anxiety
Part 3 – Bipolar Disorder
Part 4 – Schizophrenia
Part 5 – OCD
Part 6 – PTSD
Part 7 – Psychosis





