

She called the pastor at 2am. She was speaking quickly, urgently, in fragments that did not quite connect. She said she had received a message. She said she had been chosen. She said the television had been speaking directly to her for three days, that she had not slept, that he needed to understand something important was happening and the church needed to know. The pastor prayed with her over the phone. He told her to rest, to read her Bible, to come and see him in the morning. He did not know that what he was hearing was a psychiatric emergency. He did not know that what she needed was not prayer and rest and a morning appointment. She needed to go to a hospital, that night.
This is the seventh in a series on "What the Church Needs to Know about Mental Health".
Psychosis is not a diagnosis in itself. It is a symptom, or more accurately a cluster of symptoms, that can occur across several conditions, including schizophrenia, bipolar disorder, severe depression, substance use, and certain physical illnesses. It describes a state in which a person's connection to shared reality has broken down in specific, identifiable ways.
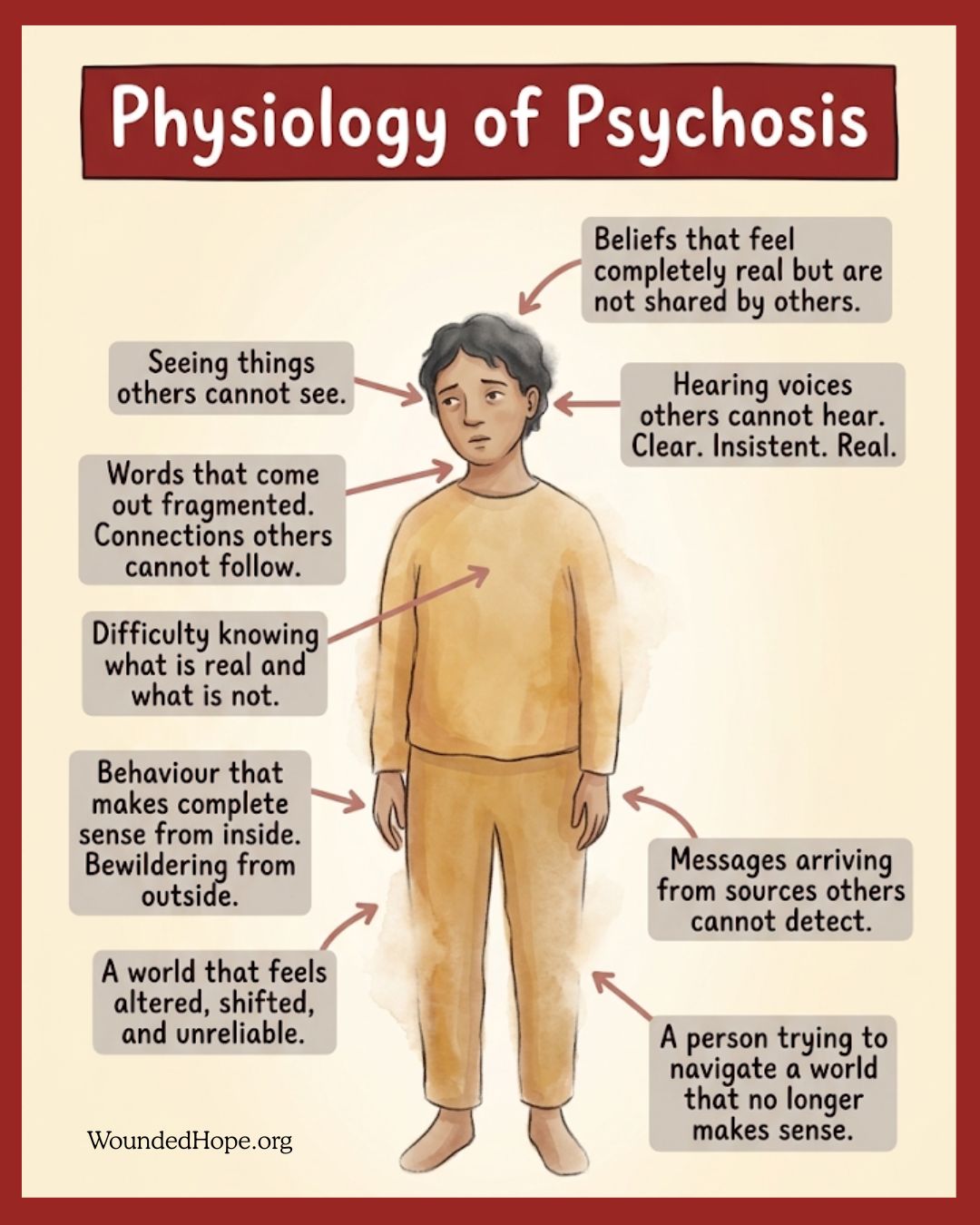
The two primary features are hallucinations and delusions. Hallucinations are sensory experiences that occur without an external cause: hearing voices others do not hear, seeing things that are not there, feeling sensations on the skin with no physical source. These experiences are entirely real to the person having them. They are not imagined or performed. The voice is heard as clearly as any other voice. The vision is seen as clearly as anything else in the room.
Delusions are fixed beliefs not grounded in shared reality, beliefs that do not yield to evidence or argument. They are often elaborate and internally coherent: that one has been chosen for a special mission, that external forces are communicating through the television or radio, that one is being watched or pursued, that one has special powers or significance. The person holding the delusion is not lying or exaggerating. They believe it completely.
Psychosis also frequently involves disorganised thinking, where the logical links between thoughts break down and communication becomes fragmented, and disorganised behaviour, where the person can no longer manage the ordinary tasks of daily life.
Psychosis is a medical emergency. That is not a dramatic phrase. It is an accurate one. An acute psychotic episode needs prompt psychiatric assessment and intervention, and delayed treatment worsens outcomes. See accompanying infographic.
The charismatic and evangelical church is especially vulnerable to misreading psychosis, for two reasons worth naming honestly.
The first is the overlap in surface presentation. A person in a psychotic episode may speak of receiving messages from God, of being chosen for a mission, of perceiving spiritual realities others cannot access. In a culture that values prophetic gifting, direct revelation, and spiritual experience, this can sound, at first, like the language of faith rather than the language of illness. The woman speaking urgently at 2am about a message and a mission may sound, in the opening moments of that call, like someone in the grip of a genuine encounter with God. A pastor who has never met acute psychosis may simply not know what he is hearing.
The second reason is theological discomfort with the medical frame. Some traditions resist psychiatric explanations for experiences that present in spiritual language, either because they believe all such experiences should be read spiritually, or because they fear a medical frame flattens the spiritual dimension of being human. Whatever its intention, that resistance has serious consequences when the experience in question is psychosis. Treating a psychotic episode as a spiritual matter requiring discernment, rather than a medical emergency requiring immediate psychiatric attention, is not only a gap in medical knowledge. It is a failure of pastoral care.
There is a further harm. When someone recovers from a psychotic episode and is told by their church that what they experienced was spiritual rather than medical, it can make staying on medication much harder. If the episode was a gift rather than a symptom, why keep taking the thing that prevents it from returning? That reasoning has contributed to relapse and hospitalisation in people with psychotic disorders, and the church bears some responsibility for it whenever it has chosen a spiritual interpretation over medical accuracy.
This is the question the church needs to be willing to ask and able to answer. How do we tell the difference between a genuine spiritual experience and a psychiatric symptom? It is not always easy. It is not unanswerable either.
The biblical tradition of prophecy has always carried discernment as a core practice. Paul tells the church to weigh what is said prophetically, instructing that others should weigh carefully what is spoken (1 Corinthians 14:29). John tells his community to test the spirits to see whether they are from God (1 John 4:1). The assumption in both is that not every experience presenting as spiritual is from God, and that the community has a responsibility to discern rather than accept uncritically.
Several things help distinguish prophetic experience from psychotic symptom. Genuine spiritual experience typically occurs in a person who is functioning normally in other areas of life, is coherent and able to communicate, does not require the abandonment of sleep, food, or basic self-care, and does not escalate over time into fragmentation and crisis. Psychosis typically involves deteriorating function, rising distress, fragmented communication, and a growing disconnection from shared reality that the person themselves often cannot perceive from the inside.
The discerning pastor is not being asked to choose between the spiritual and the medical. They are doing what the tradition has always required: testing carefully, responding wisely, and in this case, recognising when the most faithful response is to call a psychiatrist rather than to pray over someone who needs a hospital.
If you have experienced psychosis. What happened was real in your experience, and the terror and confusion of a psychotic episode are not small things. Recovery takes time and it is not linear. The medication matters. The appointments matter. The ordinary rhythms of sleep, food, and community matter more than they may seem to. You are not spiritually compromised because you experienced psychosis. You are not less known by God because your mind lost its grip on shared reality for a time. The man among the tombs was restored to himself and returned to his community (Mark 5:15), and that restoration is still the shape of the hope available to you.
If you are a family member or carer. What you witnessed during the episode was frightening, and what you are carrying afterwards is heavy. You need support specific to your situation: carers groups, psychoeducation about the condition, and honest conversations with the psychiatric team about what to watch for and how to respond if it happens again. Build an action plan with the clinical team before the next crisis rather than during it. Learn the signs of relapse. Know the number to call. Understand that what the person needs from you in the acute phase and what they need in recovery are different things. And let yourself ask for help for your own sake, not only for the person you love.
If you are a pastor or church leader. This is the condition in this series that most urgently asks you to know what you do not know. You will encounter psychosis in ministry. It may come at 2am on a phone call, surface in a prayer ministry session, or emerge gradually over weeks in someone you know well. You do not need to be able to diagnose it. You need to be able to recognise that something may be medically serious, to resist the pull to interpret it spiritually before it has been assessed medically, and to act quickly. Build a relationship with a local psychiatric or crisis service before you need it. Know the number. Know what to say when you call. Learn how to accompany a family to an emergency assessment without taking over and without minimising. And when someone recovers and comes back, receive them the way the community was meant to receive the man among the tombs, restored and in their right mind, and welcome them home.
She was hospitalised three days after the 2am call. The episode had kept escalating. By the time her family brought her in, she had not slept in five days and the fragmentation was complete. She recovered slowly, over several months. She came back to church eventually, quieter than before, sitting near the back, not quite sure of her welcome.
The pastor had done his best, and he had not known what he was hearing. He knows now. He has read what he needed to read, spoken to the people he needed to speak to, and added a number to his phone that he hopes he never has to use and knows he might. He has also learned to say, when something does not fit the categories he was trained in, that he does not know what this is, and that not knowing is not a pastoral failure. It is the beginning of a faithful response. The church does not need to have all the answers. It needs to know when to call for the ones who do.
Part 1 – Depression
Part 2 – Anxiety
Part 3 – Bipolar Disorder
Part 4 – Schizophrenia
Part 5 – OCD
Part 6 – PTSD
Part 7 – Psychosis





